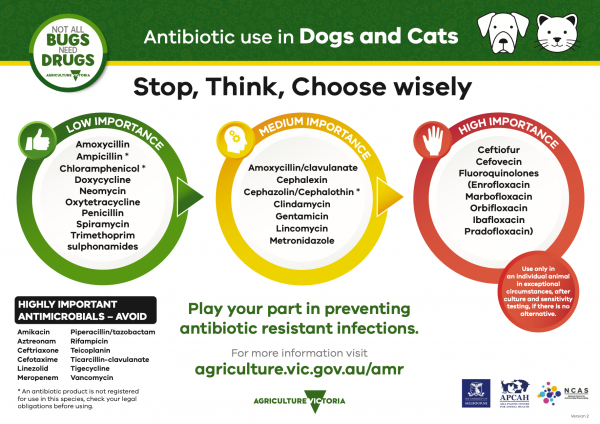
Traffic light - dogs & cats
A document that outlines via a traffic light system, the different importance level of antimicrobials for use in dogs and cats.
The surgical guidelines have been developed for all veterinarians, to inform clinical decisions, in response to a survey we completed in 2016 that identified a need for widely accessible antimicrobial guidelines for surgical prophylaxis.
The results of this survey have been published and the paper can be found at this link.
We suggest you download the VPG guidelines poster, display it in your clinic and record your protocols for surgical prophylaxis in the space provided.
Measuring compliance with the guidelines, or your clinic policy, is a powerful tool in improving appropriate antimicrobial use. Periodic review of clinical records, or review of surgical checklists, with regular reporting will motivate all staff to improve appropriate antimicrobial use for surgical prophylaxis.

To provide guidance on need for antimicrobials for surgical prophylaxis to mitigate the risk of surgical site infections and where antimicrobials are indicated, guidance on antimicrobial selection, timing and duration of therapy. We aim to provide guidance for common surgical conditions in dogs and cats, however, some conditions may not be covered and clinicians are advised to use their best judgement in these instances.
Surgery classification | Description | Examples |
|---|---|---|
| Clean | Non-traumatic, uninfected. No break in aseptic technique, no inflammation encountered. Elective, closed primarily and no drain used. | Eg Routine spey or castration Exploratory laparotomy (not entering viscus) |
| Clean-contaminated | Controlled entering of a hollow muscular viscus, minor break in aseptic technique | Eg Exploratory laparotomy for foreign body removal, cystotomy (no abdominal contamination) |
| Contaminated | Open, fresh traumatic wound. Incision into a site with acute, non-purulent inflammation. Major break in aseptic technique. | Eg Cystotomy/laparotomy with significant abdominal contamination, pyometra, closure of contaminated traumatic wound (<4h duration). |
| Dirty | Pus encountered during surgery. Perforated viscus found. Traumatic wound with devitalised tissue, foreign material or faecal contamination, or of more than 4-hour duration. | Eg Peritonitis, necrotic traumatic wound (>4h duration) undergoing primary closure. |
| Surgical contamination level | Complicating factors | Likely pathogens | Antimicrobial recommendation | Duration of therapy | Level of evidence |
|---|---|---|---|---|---|
| Clean | None1 | N/A | None | Strong | |
If surgical site infection would be a major threat to the patient (ie central nervous system surgery) Hypotension Surgical duration >90 mins3,4 Obese dogs5 Endocrine disorder6 Bacterial dermatitis | Amoxycillin or 1st generation cephalosporin | Stop within 24h*2 | Medium | ||
| Implant1,7 | Orthopaedic: Staphylococcus intermedius | Amoxycillin or 1st generation cephalosporin | Perioperative only**7 | ||
| Clean contaminated | Gastrointestinal | Coliforms, anaerobes if caudal GI tract | Amoxycillin or 1st generation cephalosporin | Stop within 24 hours* | Medium |
| Contaminated | Pyometra, prostatic abscess | E. coli, Streptococcusspecies, Anaerobes | Amoxycillin or 1st generation cephalosporin & gentamicin & metronidazole | No evidence, 24-48 hours is common in human medicine | Weak |
| Significant bowel leakage | Coliforms | Amoxycillin & gentamicin | No evidence, 24-48 hours is common in human medicine | Weak | |
| Dirty | Choose appropriate for infection (ideally based on culture and susceptibility testing) | Until clinical signs resolve | Weak | ||
| Dental | None | None | None | N/A | Medium |
Geriatric patients Heart disease Systemic illness Immunosuppression | Bacteraemia expected for duration of procedure8, 9. If cannot tolerate this: clindamycin or amoxycillin. | Stop within 24 hours* | Weak |
* Stop within 24 hours indicates administration prior to and during surgery, and doses after surgery up till 24 hours. Inter-dosing interval after surgery is described below.
**Perioperative only indicates administration prior to and during surgery, but no further doses after surgery
Tissue levels of antimicrobials are required at the time of first incision to confer protection from surgical site infection.
Intravenous antimicrobials: administer 30-60 mins prior to surgery
Subcutaneous amoxycillin / clavulanate: 2 hours prior to surgery
Tmax for individual drugs given by different routes can be used to assess optimal timing to achieve peak serum levels at the time of first incision.
Dosing interval should be measured from the time of the preoperative dose. The dosing interval during surgery can be calculated as twice the elimination half-life of the antimicrobial. For example, the dosing interval during surgery for common intravenous antimicrobials used in surgery for dogs and cats are:
Cefazolin: Maintains concentrations above MIC for common skin pathogens (Staphylococcal & Streptococcal species) for 4 hours (10),however 2 hourly administration (twice elimination ½ life) may be required for E.coli. (11)
Amoxycillin: 2 hours
Following surgery, if antimicrobials continue to be indicated, the dosing interval returns to that used for non-surgical indications.
Clip hair less than 4 hours before surgery4
Minimise number of people in surgical theatre5
Consider use of surgical safety checklist. Use of these tools has reduced surgical complications from 17% to 7% (SSIs from 5% to 1.4%).11
(Based on World Health Organisation surgical safety checklist)
These guidelines are designed to be evidence-based and transparent. As such, we’ve provided the evidence behind our recommendations.
A literature search was undertaken in PubMed using the following search terms:
(Dog OR Cat OR Canine OR Feline) AND Surg* AND (Antibiotic OR Antimicrobial OR Infection OR Complication)
Only research papers pertaining to species other than humans, with abstracts, and papers written in English were considered. No time limit was included.
In addition, guidelines from other professional organisations (restricted to those written in English) were reviewed and in particular, the reference lists of these guidelines. Only evidence-based recommendations were considered in constructing these guidelines. The guidelines were created by consensus by the development group.
The abstracts for all returned articles were examined. Articles were included if the title or abstract suggested that either surgical site infection or antimicrobial prophylaxis for surgery were discussed in the paper. In addition, articles were excluded if the sample size was insufficient to make appropriate inferences from the study. All study designs were considered as the literature is limited.
| Research setting | SSI | Type of surgery | Comments |
|---|---|---|---|
| Private practice, Canada19 | 1-4% | OVH & castration | |
| University practice20 | 12.70% | OVH | |
| University practice21 | 2.50% | Elective | |
| University practice2 | 3.60% | CCL | |
| University practice22 | 3.90% | CCL | Perioperative antimicrobials did not influence rate although only small number that didn’t get antimicrobials |
| University practice4 | 1.70% | Minimally invasive | |
| University practice4 | 5.50% | Open surgery | Perioperative antimicrobials did not influence rate |
| University practice21 | 2.50% | Clean | |
| University practice21 | 4.50% | Clean-contaminated | |
| University practice21 | 5.80% | Contaminated | |
| University practice21 | 18.10% | Dirty | |
| University practice23 | 4.50% | Clean | |
| University practice3 | 0.80% | Clean | |
| University practice24 | 3.50% | Elective joint surgery | |
| University practice25 | 9.0% | External fixation in cats |
OVH, ovariohysterectomy; CCL, cranial cruciate ligament syndrome.
| Domains Confounding | Selection bias | Classification bias | Deviation from intended intervention | Missing data | Measurement | Reporting | Reason for non-inclusion | |
|---|---|---|---|---|---|---|---|---|
| Aiken et.al. 20177 | 0 | 0 | 0 | + | 0 short and medium term ++ long term | 0 | 0 | |
| Andrade et.al. 201626 | +++ | + | 0 | N/A | 0 | 0 | 0 | Risk of confounding too high |
| Beal et.al., 200027 | + | + | 0 | NR | 0 | + | 0 | |
| Beever et.al., 201725 | + | 0 | 0 | N/A | + | + | 0 | |
| Bergstrom et.al., 201611 | + | + | 0 | 0 | Not assessable | + | 0 | |
| Billings et.al., 199024 | +++ | ++ | 0 | 0 | Not assessable | Not assessable | N/A | Risk of confounding too high |
| Bristow et.al., 201528 | ++ | + | 0 | NR | Not assessable | Not assessable | N/A | Did not report length of antimicrobial therapy |
| Bowersock et.al., 20008 | 0 | 0 | 0 | 0 | 0 | 0 | + | |
| Casale & McCarthy, 200922 | + | ++ | 0 | N/A | NR | + | N/A | |
| Cook et.al., 201014 | + | + | 0 | 0 | Not assessable | Not assessable | 0 | |
| Eugster et.al., 20045 | 0 | 0 | 0 | N/A | + | + | 0 | |
| Fitzpatrick & Solano, 201015 | +++ | + | 0 | 0 | Not assessable | + | 0 | Pre-operative antimicrobial therapy not given early enough |
| Frey et.al., 201018 | + | ++ | 0 | 0 | Not assessable | Not assessable | N/A | Did not report length of antimicrobial therapy |
| Gatineau et.al., 201116 | +++ | +++ | 0 | N/A | Not assessable | Not assessable | 0 | Did not report timing of antimicrobial therapy, post-operative therapy given at the surgeon’s discretion |
| Heldmann et.al., 199923 | ++ | +++ | 0 | 0 | Not assessable | Not assessable | N/A | Did not describe antimicrobial therapy |
| Jardel et.al., 201129 | +++ | +++ | 0 | 0 | Not assessable | Not assessable | N/A | High risk of confounding and selection bias |
| Nazarali et.al., 201430 | ++ | +++ | 0 | N/A | NR | 0 | ++ | High risk of confounding, selection and reporting bias |
| Mayhew et.al., 20124 | ++ | ++ | 0 | N/A | + | 0 | N/A | |
| Nicoll et.al., 201431 | 0 | 0 | 0 | N/A | 0 | 0 | N/A | |
| Nicholson et.al., 20026 | ++ | ++ | 0 | N/A | NR | 0 | +++ | Limited data in paper to verify results. No reporting on effect of antimicrobials |
| Nieves et.al., 19979 | 0 | 0 | 0 | N/A | 0 | 0 | + | |
| Pacchiana et.al., 200317 | +++ | + | 0 | N/A | Not assessable | Not assessable | 0 | Antimicrobial therapy given at the discretion of surgeon and not included as exposures variable |
| Pratesi et.al., 201532 | 0 | 0 | 0 | + | 0 | 0 | +++ | |
| Pollari & Bonnett, 199618 | 0 | + | + | N/A | 0 | + | 0 | |
| Solano et.al., 201533 | +++ | +++ | 0 | NR | NR | 0 | + | Confounding and selection bias too high |
| Stauffer et.al., 200613 | 0 | + | 0 | N/A | NR | 0 | N/A | |
| Turk et.al., 20151 | 0 | 0 | ++ | N/A | NR | ++ | 0 | |
| Vasseur et.al., 19853 | 0 | 0 | 0 | NR | N/A | 0 | 0 | |
| Vasseur et.al., 198821 | ++ | 0 | + | N/A | NR | + | N/A | |
| Weese & Halling, 20062 | + | + | 0 | N/A | Not assessable | 0 | N/A | |
| Yap et.al., 201512 | + | + | 0 | N/A | Not assessable | Not assessable | 0 |
Risk of bias was assessed using the ROBINS-I assessment tool28.
NR, not reported; N/A, not applicable
Manuscripts in red were not considered for recommendations.
Range 0 (no bias detected) to +++ (major bias detected)
A document that outlines via a traffic light system, the different importance level of antimicrobials for use in dogs and cats.
The companion animal Australian Veterinary Prescribing Guidelines for antimicrobial use in flipbook format.

The companion animal Australian Veterinary Prescribing Guidelines poster. This document that outlines different antimicrobials for use in dogs and cats according to different diseases.
Suggest a disease, syndrome or key evidence you think we should include.