
Traffic light - Horses
A document that outlines via a traffic light system, the different importance level of antimicrobials for use in horses.
This page outlines antimicrobial use guidelines for the diagnosis and management of dermatological, wounds and foot disorders in horses.

Equine thermal injuries may result from barn fires, bushfires, grass fires, contact with hot solutions, electrocution or lightning strike, friction (e.g. rope burns), abrasions or chemicals.There are some important differences between the impact and types of injuries sustained during barn fires compared to bushfires. In grass fires and bushfires, burns are usually located on the extremities and ventral abdomen, whereas in barn fires, dorsal thermal injuries are more common (2).The literature on the management of equine thermal injuries is predominantly based on injuries sustained during barn fires, with little information available about the types of injuries sustained during bushfires (2, 3).
The most common pathogens causing secondary infections in burn wounds are Staphylococcus aureus and Pseudomonas aeruginosa (4).
A thorough patient assessment is important prior to the instigation of treatment of thermal injuries, paying particular attention to cardiovascular function, pulmonary status, ocular lesions and the extent and severity of the burns (1).
The extent of the burn depends on the size of the area exposed, whereas the severity is determined by the maximum temperature the tissue attains and the duration of overheating (1). The percentage total body surface area affected usually correlates with mortality, whereas the depth determines morbidity (1).
There are several physical criteria used to evaluate burns, including erythema, oedema and pain, blister formation, eschar (slough produced by a thermal burn) formation, the presence of infection, body temperature and cardiovascular status (1).Erythema, oedema and pain indicate the presence of some viable tissue and are therefore favourable signs. However, pain is not a reliable indicator for determining burn depth. An accurate evaluation of the severity of a burn often cannot be made until there has been time for further tissue changes (1).

Figure 14.1 Progression of wounds following severe thermal injuries (3rd degree).
Burns are classified by the depth of injury, with first-degree burns involving the most superficial layers of epidermis.Second-degree burns may be superficial (basal layers remain relatively uninjured) or deep (all layers of the epidermis). Third-degree burns involve loss of the epidermal and dermal components and are accompanied by extensive fluid loss, lack of pain, and eschar formation. Fourth-degree burns involve all skin and underlying muscle, bone, ligaments, fat and fascia (1).
It is important to identify injury to major vessels of the lower limbs and the presence of eye, perineal and synovial structure involvement. Signs of ocular/corneal damage include blepharospasm and excessive lacrimation. The presence of a cough may indicate smoke inhalation, and this is often a predominant feature of thermal injuries sustained in barn fires due to exposure to a large accumulation of smoke in a confined/closed space.

Figure 14.2 Wound contracture after Grade 3 burns to the head of a 3 year old Quarterhorse filly at 19 days, 29 days and 2 months after the initial injury.
Horses may present with clinical signs consistent with a systemic response to thermal injuries, including tachycardia, fever and injected mucous membranes. Haematological and serum biochemical analysis is useful to assess the systemic response and to identify the presence of organ dysfunction, which may develop because of systemic inflammation, generalised hypoxia and/or severe cardiovascular and haemodynamic compromise. Abnormalities reported in horses with thermal injuries include a low total protein concentration and anaemia that can be marked and gradually progressive. This is initially caused by immediate red blood cell (RBC) destruction by heat and wound haemorrhage with subsequent RBC loss from intravascular and extravascular removal of damaged cells (1).Haemoglobinuria can also develop and platelet aggregation on damaged capillary endothelium can result in thrombocytopaenia (1).
Other diagnostic tests that can be considered in cases of thermal injury include a clotting profile, urinalysis, arterial blood gas analysis, thoracic radiography and bronchoalveolar lavage (BAL).
Initial Stabilisation
Severe burns can lead to dramatic cardiovascular effects, often referred to as ‘burn shock’. This resembles hypovolaemic shock (1).A combination of vascular responses ultimately results in an accumulation of fluid, protein and inflammatory cells in the wound. There is also fluid loss into the extravascular space, which leads to an acute reduction in blood volume. The extent of fluid loss is determined by the severity of the burns, and fluid losses will result in increased heat loss from evaporation and an increased metabolic rate (1).
Initial patient stabilisation involves fluid support for the acute haemodynamic alterations that can occur in these cases, as well as immediate cooling to halt the burn process (3). Fluid resuscitation is important in avoiding the sequelae of haemodynamic shock, including decreased gastrointestinal and renal perfusion.
Wound management
The local care of burns generally involves halting the burning process, cleansing and debridement, and application of topical ointments and/or dressings to support healing. The use of cold water (2 - 15°C) treatment as first aid for burns has the greatest volume of supporting evidence, compared to using ice, which may lead to a thicker eschar and may worsen ischaemic necrosis (5). Mild natural soaps (e.g. Sunlight soap) are recommended for wound cleansing and to aid in softening and removal of dead skin. Other soaps and cleansers containing dilute chlorhexidine and/or betadine/iodine should be avoided as they may cause skin irritation.
Although bandaging is the standard of care in the management of burns in human patients, bandaging may not be well tolerated by horses. Pruritis is common during the wound healing process and continual scratching can cause bandages to slip. The use of single layer compression bandages is often much better tolerated and can also reduce distal limb oedema and the amount of exudation from wounds (see Case Study and Figure 14.3).
Pain management
With the severe tissue injury that occurs with thermal injuries, physiological pain can evolve to a state of pathological pain if not appropriately managed. Multimodal pain control is often considered most appropriate, as it has the advantage of additive or synergistic analgesic effects and also allows for the use of lower doses of individual analgesic agents to limit the adverse side effects. An example of agents that may be utilised in a multimodal pain management protocol for thermal injuries is summarised in table 14.1 below. See the case study in this chapter for a specific protocol used on a patient with a mixture of 1st, 2nd and 3rd degree burns to 30% of their body (Figure 14.3).
Table 14.1. Multimodal pain management protocol for thermal injuries*
Drug or drug class | Route | Dose | Comments |
NSAIDS | Oral or IV | Specific to drug | |
Lignocaine | CRI | Bolus of 1.3 mg/kg then 0.05 mg/kg/minute | Overdose may result in seizures or CNS excitation. May be used for several days. |
Ketamine | CRI | 0.4 - 1.2 mg/kg/h | Ataxia and sensitivity to sound possible at higher doses. May be used for days to weeks. |
Opioid morphine OR butorphanol | CRI CRI | Loading dose of 0.3 mg/kg, then 0.05 mg/kg/h Bolus of 17.8 µg/kg then 10-15 µg/kg/h | Should give the loading dose with an alpha-2 agonist (eg. detomidine) to prevent excitement. May impact gastrointestinal motility. Tolerance may develop, usually used for 12-24h |
Alpha-2 agonists | IV or IM | Specific to drug | |
Paracetamol | PO | 20 - 25 mg/kg q 12 h | |
Gabapentin | PO | 20 - 60 mg/kg q 12 h | Poor bioavailability so high dose required. Mixing crushed tablets with oil (e.g. corn oil) can make administration easier. |
* Not all horses will need all medications in this list.
The use of systemic antimicrobials is not warranted to protect against wound infection in horses with thermal injuries. They cannot penetrate the avascular eschar, where the risk of contamination is greatest (1). In addition, circulation to the burned area is often compromised, making it highly unlikely that parenteral administration of antimicrobials can achieve therapeutic concentrations at the wound. Systemic antimicrobials do not favourably influence wound healing, fever or mortality and can also facilitate the emergence of resistant microorganisms.
The warm, moist site of a burn wound is an ideal environment for bacteria to multiply. Topicalantimicrobials can prevent the conversion of superficial wound sepsis to full-thickness infection and possible systemic sepsis (1). Examples of topical antimicrobials used include:
The prognosis depends on the systemic condition of the patient and the extent, depth and location of the thermal injuries. The proportion of the total body surface area affected usually correlates with mortality, while the depth of the burn determines the morbidity (1).If > 50% of the body surface is affected, euthanasia is recommended.
Minor first-degree and superficial second-degree burns are easily managed in the field, while extensive first- and second-degree burns, and third- and fourth-degree burns, are usually best managed by referral to an institution where the level of intensive care required is available. Long-term care is required to prevent continued trauma and the associated pruritis needs to be managed.
The prognosis will also depend on the development of secondary injuries and/or complications (e.g. laminitis, colic, colitis).
The term cellulitis refers to diffuse infection of the subcutaneous tissues. In horses, cellulitis involving the limbs is typically acute in onset and characterized by substantial inflammation, swelling, heat and pain. Lameness is variable, but non-weight bearing (5/5) or substantial lameness at the walk (4/5) is common. Cellulitis can be primary or secondary, and the underlying cause is often unknown, although it can develop associated with soft tissue trauma and concomitant inoculation of bacteria. The common primary causes of secondary cellulitis include wounds, surgical incisions and intra-articular medication (8). Regardless of whether it is primary or secondary, cellulitis is a serious condition and can be frustrating for both veterinarians and owners when it is recurrent. In addition, severe complications, such as dermal necrosis, laminitis and vascular thrombosis, have been reported. Coagulase-positive Staphylococcus spp. (followed by Streptococcus spp. and E. coli) seem to be the bacteria most commonly isolated from cases of primary cellulitis and Streptococcus spp. (followed by coagulase-positive Staphylococcus spp. and Pseudomonas spp.) the bacteria most commonly isolated cases of secondary cellulitis in the UK (8), but no data are available from Australia.
Diagnostics
Diagnosis is usually based on clinical signs, but additional diagnostics may be useful. Ultrasonographic examination may be useful, especially to identify areas of fluid accumulation for sampling for further diagnostic investigation. Haematology generally reveals a leukocytosis (usually without a left shift) and hyperfibrinogenaemia. Given the common organisms have susceptibility patterns that are unpredictable (Staphylococcus spp., Pseudomonas spp.), culture of fluid collected from pockets in affected areas and susceptibility testing of bacterial isolates is recommended.
NSAIDs (most commonly phenylbutazone) and systemic antimicrobials are the mainstay of treatment. Empirical therapy is generally with either penicillin and gentamicin or trimethoprim/sulphadiazine. In mild to moderate cases, oral, intravenous or intramuscular administration of antimicrobials is likely to be sufficient and the duration of therapy is typically five days. Three days may be adequate for mild cases. Resolution of clinical signs can be used as an indication that antimicrobial therapy can be discontinued.
In severe cases, intravenous regional limb perfusion (IVRP) should be considered (See Section 12). In extensive cases, IV access for IVRP may not be possible and should not be attempted through affected tissue as septic thrombophlebitis can result. IVRP with gentamicin is most appropriate and 1/3 of the systemic dose is recommended. (See the IVRP guideline in Section 12 for more details.) The perfusate volume does not seem to affect antimicrobial concentrations in the limb, but a pneumatic or wide rubber (12.5 cm) tourniquet should be used (9).
Ancillary treatment is also helpful. Cold water hosing, compression bandaging and light exercise (walking) can all help to reduce oedema and prevent dermal necrosis.
In secondary cases, especially following intra-articular injection or intrasynovial surgery (arthroscopy or tenoscopy), septic synovitis should be considered.
In mild to moderate cases, the prognosis is good.
In severe cases, the prognosis is guarded. Cases that develop laminitis have a worse prognosis and horses with fever tend to be more severely affected (8).
Summer sores typically occur in pre-existing wounds, but can occur on the commissures of the lips, the medial canthus of the eye, the nasolacrimal ducts and the prepuce/urethra of stallions or geldings (muco-cutaneous habronemiasis). The onset is often characterised by the rapid development of papules or the failure of a wound to heal, and the development of exuberant granulation tissue. Ulceration, intermittent haemorrhage and a serosanguinous exudate are also common. Pruritis is variable. Small (1 mm diameter) granules may be seen within the affected tissue, which are necrotic, caseous-to-calcified foci surrounding nematode larvae. In contrast to the lesions seen in pythiosis, the granules do not branch.
The chest, fetlocks and the medial surface of the legs are the most commonly affected areas on the body. Lesions may heal, or recurrent lesions may evolve into non-healing granulomatous cancer-like masses that attract more flies, leading to a super-infection. Wounds tend to disappear spontaneously in the cold months, but re-appear when the environmental temperature rises again months later.
The lesions are caused by the larvae of the nematodes Habronema muscae and Draschia megastoma, less commonly Habronema microstoma. The differential diagnoses include exuberant granulation tissue, squamous cell carcinoma, sarcoids and pythiosis.
Adult Habronema muscae are found in the stomach, causing minimal problems. The mature worms lay their eggs, which are passed in the manure. The eggs are consumed by stable fly larvae and are normally deposited near the mouth of the horse, where they are swallowed and develop in the stomach, completing their life cycle. However, when the larvae are deposited onto a wound they cannot develop further and migrate through the tissues, causing intense itching. The self-trauma caused by the itching contributes to the size of the lesion.
Histological examination of affected tissue is generally diagnostic. The wounds are infiltrated with eosinophils, macrophages, lymphocytes and a few plasma cells. In peripheral areas, an abundance of vascular and fibro-connective tissue can be observed, with masses of eosinophils in areas of coagulative necrosis. Sections of nematodes can be also detected. However, the larvae tend to be few and may have been digested or be necrotic in more chronic lesions. Larvae live for < 1 month in cutaneous tissues, and larval death may cause even more necrosis and calcification than when alive. The diagnosis may be challenging when sarcoid and habronemiasis occur concurrently.
Many treatment regimens have been described, and no “optimal” therapy can be recommended. The therapeutic strategy will depend on the chronicity, the size and location of the lesions, as well as financial considerations and practicality for clients, but typically includes local and systemic therapy. Surgical debulking intervention is indicated in large and more chronic wounds or when the medical treatment of summer sores is refractory, although other differential diagnoses should be considered in these cases.
Ivermectin (0.2 mg/kg PO) and moxidectin (0.4 - 0.5 mg/kg PO) are both very effective larvicides and have wide margins of safety. Two doses are given at a 21-day interval.
Systemic glucocorticoids have been found to be very effective as the sole systemic agent in equine habronemiasis and have also been used to reduce pruritis following antiparasitic therapy. Prednisolone (1 mg/kg PO every 24 h), dexamethasone (0.04 mg/kg PO), or intralesional triamcinolone (10 - 20 mg/lesion) results in a marked resolution of most lesions within 7 - 14 days. Topical steroids have also been used, along with many other different topical therapies, usually in combination, and, given that some summer sores regress spontaneously, it is difficult to infer the efficacy of any product.
Any topical treatment should be applied under a bandage to prevent the deposition of new larvae during the healing process. When bandaging is not possible, a fly repellent ointment should be applied.
Good for small to medium sized lesions. Guarded for extremely large or chronic lesions.
Poorly fitting tack may cause friction and pressure sores that result in pain and skin injuries. Prolonged, continuous pressure — often relatively mild — leads to ischaemic necrosis. Ill-fitting bandages and casts, prolonged anaesthesia/surgical procedures, and prolonged recumbency can also lead to ulcers. Mixed bacterial infections of ulcers occur secondarily.
The diagnosis is based on the history and physical examination.
Early signs include:
If untreated, the injured area will progress to ulcers that tend to be deep and become secondarily infected and cause pain, most commonly on the withers. The ulcers tend to be very slow to heal. Scarring and leukotrichia after healing are common.
The most important aspect of therapy is to identify and correct the cause. Routine wound care includes daily cleansing and drying agents, and topical antiseptics. Systemic antimicrobials are virtually useless. Surgical debridement, surgical excision or skin grafting may be necessary. Prevention is vastly superior to any kind of therapy.
Good when primary cause is addressed, although recovery can be slow.
Dermatophilosis (rain scald) is one of the most common bacterial infections of equine skin worldwide and yet studies on its treatment are uncommon. It is caused by Dermatophilus congolensis, a Gram-positive, facultatively anaerobic, branching filamentous rod with a distinctive appearance. Infections cause a superficial pyoderma that can be acute or chronic.
D. congolensis is an opportunist pathogen of the skin of infected horses. Transmission is by direct contact with infected animals, contaminated environments (like shared blankets or grooming tools), and possibly via insects. Factors that suppress the host’s immune system, such as concurrent disease and/or stress, may enable the organism to proliferate and produce clinical disease. However, lesions most commonly develop when the skin is exposed to chronic moisture, such as when wet horses are rugged.
Clinical signs of dermatophilosis include a mildly painful, non-pruritic superficial pyoderma with regional or generalized papules and crusts that can resemble small paintbrushes when lifted. A yellow/green exudate is commonly present under the crusts in early lesions, which occur most commonly on the dorsum, face and neck. In very severely affected horses, and those with secondary bacterial infections, fever, depression, lethargy, and anorexia may be present and some may have a regional lymphadenopathy, but this is rare. Most diagnoses are made on clinical signs alone.
Dermatophilosis is diagnosed by demonstration of the distinctive branching filamentous rods in direct smears of the exudate, in histopathological sections, or in a preparation made from dried or fresh crusts. Cytological examination of samples of exudate or rehydrated crusts reveals the classical “railroad track appearance” of longitudinally arranged coccoid zoospores (figure 14.4). If performing a skin biopsy, it is important to submit a specimen with the crust attached to the skin or hairs. The organism is often found only in crusts, and, if needed, the crust can be submitted instead of a full biopsy specimen if the history, signalment and physical examination support a diagnosis of dermatophilosis, but this is rarely required to make a diagnosis.
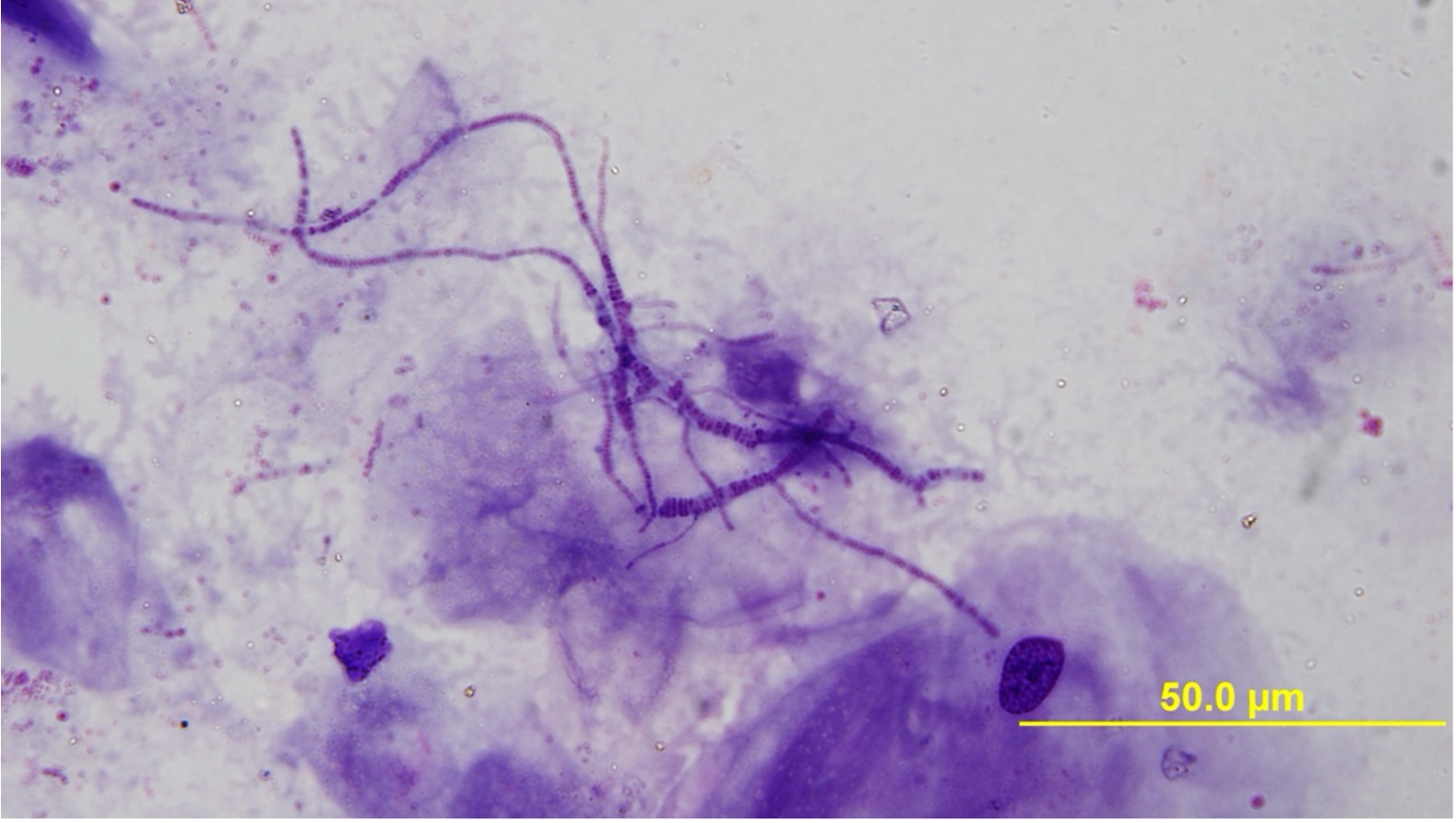
Figure 14.4. Classic ‘railroad track’ appearance of dermatophilosis on cytology. (Giemsa stain. Image courtesy of J. Norris.)
Topical therapy is generally successful in horses with mild to moderate infections. The bacteria seek carbon dioxide and the layering and crusts created by the exudative host response provide a protective environment. Thus, removal of the crusts is essential for treatment. Crusts are gently soaked and removed while bathing with a mild antibacterial shampoo, such as one containing chlorhexidine. For some horses this is quite painful and may require sedation. Drying the skin is important. Severely affected animals may require systemic antimicrobial treatment to lift the crusts, such as administration of procaine penicillin at 22,000 IU/kg IM twice daily for 2-3 days. Trimethoprim/sulfadiazine (TMS) at 30 mg/kg orally twice daily for 2-3 days also may be effective.
Regardless of all other treatments, exposure to excessive moisture must be controlled.
Good when skin moisture can be controlled.
Staphylococcal folliculitis and furunculosis (acne, heat rash)
Cases most commonly start in spring and early summer, which is likely to be because of the coat shedding, clipping, heavy riding and work schedules, higher environmental temperatures and humidity, and increased insect population densities that occur during this time of year. However, there are many predisposing causes (e.g. hypersensitivities, ectoparasites, trauma), so lesions can occur at any time of year.
The sides of the neck, the saddle region, rump and shoulders are commonly affected. The superficial lesions of folliculitis are usually asymptomatic, while the deep lesions of furunculosis are often painful. Pruritis is not usually present. If triggering factors are not addressed, recurrences are common.
The diagnosis is usually based on history and physical examination. Cytology, culture, and/or examination of biopsies can be used to confirm the diagnosis.
Frequently, the first sign is erect hairs over a 2 to 3 mm diameter papule that is more easily felt than seen. Small crusts may also be present. These lesions can regress spontaneously, but often enlarge progressively. Some lesions enlarge to 0.5 – 1 cm in diameter, develop a central ulcer that discharges a purulent or serosanguineous material, and then become encrusted.
Treatment/elimination of underlying or associated disorders is critical to a successful outcome. Clip, clean and establish drainage. Treat topically. Cleaning of all tack, grooming equipment, blankets, and other equipment may be necessary.
Mild, superficial infections may resolve spontaneously, but most require therapy with topical cleansing, drying and antibacterial therapy. Topical applications of chlorhexidine, as a shampoo for widespread infections, daily for 5 - 7 days, is generally successful, especially if the scabs are removed effectively in the early stages. Mupirocin ointment may be useful for localised superficial or deep infections.
Severe furunculosis may require combined topical and systemic antibiotic therapy. Staphylococci have unpredictable susceptibility patterns, so empirical recommendations are difficult and therapy should be based on culture and susceptibility testing results. Trimethoprim/sulfadiazine is commonly used as first line therapy. Antimicrobial therapy is continued until clinical resolution of disease is seen.
Good when the primary cause is addressed.
Equine pastern dermatitis (EPD) is a term used to describe inflammatory cutaneous lesions on the lower legs of horses. There are numerous lay terms for these lesions, including “scratches,” “mud fever,” and “greasy heel.” In lighter breeds, mild to moderate disease is most common, while the severe form is most commonly seen in cob and draft-type horses. Although three forms have been described, the disease presents across a continuum, rather than categorically. The mildest form is characterised by alopecia, dry scales and crusts, without pain or pruritis. With increasing severity, lesions become exudative and form crusts, and may extend beyond the pastern. In advanced and chronic cases, hyperkeratosis, lichenification and fissured skin, sometimes with hyperplasia, fibrosis and excessive granulation tissue, can involve large areas of the distal limb. Pain in these cases can be considerable and lameness is common. Lesions can be constantly present, appear acutely or recur after phases of remission (17). Risk factors include feathered limbs, unpigmented pasterns (in light horses, but not in heavy breed horses). Although no genes for susceptibility have been identified, a genetic link seems likely, particularly in heavy breed horses. Chronic wetting of the skin and unhygienic conditions also promote EPD. Infestation with Chorioptes bovis is the most frequently cited parasitic cause in draft and cob/pony breeds, but is not reported as a cause in lighter breeds. Bacterial involvement is likely opportunistic. Most studies including bacterial culture have detected mixed flora or a range of bacterial species, with staphylococci and b-haemolytic streptococci isolated most commonly. Drug resistance appears uncommon.
A complete history should include investigation of the signalment, onset and course of clinical signs, seasonality, signs of disease in companion horses, previous treatment and the outcome of these treatments. An assessment of housing and environmental management is also important to identify potential risk factors.
Crusts, scales, thickened skin, ulceration and pruritis are all common signs. There are several scoring systems for assessing lesions and these may be useful in cases where lesions are constantly present (18). However, none of the scoring systems have been validated outside of the institution where they were developed, and none have been uniformly adopted in Australia.
In feathered horses, clipping is critical for proper examination of the skin lesions. Sedation and soaking of crusts may be required before clipping is tolerated. In ongoing or recurrent cases, superficial swab or tissue samples should be collected for bacterial and fungal culture, and impression smears collected for cytological examination. Many aetiologies are possible and they all are clinically indistinguishable. If photosensitivity is suspected, a serum chemistry panel should be performed to investigate whether there is primary hepatic disease.
Environmental management is key and includes avoiding wetness and humidity around the affected skin, improving pasture and stable hygiene, or cleaning and drying legs following turnout. Feathers are an important predisposing factor, so they should be clipped to decrease moisture retention and allow for effective treatment, regular inspection and maintenance of hygiene.
Sedation may be required to facilitate initial treatment. There have not been any controlled trials of commonly used treatments. Topical preparations should include initial cleaning to remove crusts, and debridement and disinfection of the lesions. Povidone-iodine should probably be avoided as it can be irritating to the skin, so chlorhexidine is preferred. Common topical preparations include agents that promote wound healing (e.g. zinc oxide, honey, colloidal silver), astringents (e.g. benzoyl peroxide) or that have hypertonic properties (e.g. magnesium sulphate), as well as antiseptic or antimicrobial agents (e.g. chlorhexidine, neomycin) and corticosteroids (e.g. betamethasone, prednisolone or hydrocortisone).
Guarded. Persistent and recurrent disease is common.
Pythiosis (swamp cancer) is a deep, invasive and rapidly progressive subcutaneous oomycotic (fungal-like) infection. The disease predominantly occurs in tropical and subtropical regions and generally during the warmer and wetter months of the year, although climate change seems to be increasing the range of regions where pythiosis occurs. It is caused by the waterborne pathogen Pythium insidiosum and can affect the skin, subcutaneous tissue and occasionally the gastrointestinal tract. The organism thrives in swampy, aquatic environments and infects horses though wounds or breaks in the skin, or after prolonged contact with contaminated water. Deep or disseminated infection may invade bone, synovial structures, the lungs and the gastrointestinal tract.
The onset is insidious, with fast-growing lesions. Common areas affected include the distal limbs, the ventral abdomen and thorax, as well as the lips, nostrils, face, external genitalia, neck and trunk. Early lesions are usually single or multiple small foci of necrosis that progress rapidly to single and large nodular eroded to ulcerative granulomas. Formation of small hard coral-like masses, called “kunkers”, is a characteristic of the disease in horses. Moderate to severe pruritis that leads to self-mutilation is a hallmark of the disease. Oozing of serosanguinous discharge is typical. Tissue necrosis leads to malodorous lesions. Severe oedema of the affected limb is also common.
Infection is locally invasive and spreads to lymphatic vessels and nodes, and deeper tissues. Osseous involvement can occur when lesions are chronic. Metastasis to the lungs may also occur.
Differential diagnoses include exuberant granulation tissue and cutaneous habronemiasis. The diagnosis of pythiosis can be made quickly by evaluation of the kunkers if they are sent to a laboratory specialising in the diagnosis of the disease. An initial diagnosis can be made grossly on lesion appearance, location, and/or the presence of kunkers. A definitive diagnosis can also be made by serology, examination of biopsies, culture, and cytological examination of exudates. Biopsies of early lesions reveal abundant microabscesses with eosinophils and a few neutrophils, lymphocytes, and macrophages. In chronic cases, an eosinophilic granuloma with giant cells is observed, with microabscesses and kunkers at the centre. P. insidiosum appears as sparsely septate hyphae 6 to 10 mm in diameter in sections or smears stained with periodic acid-Schiff or silver.
Surgical excision has been the most commonly performed therapy, but recurrence is common (up to 30% of cases) and surgical excision is difficult on limbs. Iodides and amphotericin B have both been used systemically. There is no theoretical basis for the use of amphotericin B (the target of the drug is missing) and systemic therapy does not greatly improve the outcome. A therapeutic vaccine has been developed in the USA and has been found successful in acute and chronic cases. This vaccine is not currently available in Australia, but there may be some Australian companies that can make autogenous pythiosis vaccines on request. The efficacy of these vaccines is unknown, but success has been reported anecdotally.
Lesions in horses are best treated with a combination of therapies, including radical surgical excision of the lesion and topical application of antifungal solutions. Systemic iodides (sodium iodide at 10-40 mg/kg per day as a 20% solution given slowly IV for 2 - 5 days, then oral potassium iodide at 20 - 40 mg/kg/day). Topical antifungals are generally used despite lack of theoretical benefit – amphotericin B or ketoconazole.
The prognosis for horses with cutaneous pythiosis is guarded, even if it is recognised early and immediately and aggressively treated. Immunotherapy may improve the prognosis if it becomes available. If surgical excision cannot be achieved, the prognosis is worse. The fatality rate is 100% if lesions are left untreated and the success of treatment declines with the chronicity of the lesions (> 1 - 2 months in duration).
Wounds are common in horses. The site of the wound, its depth and the involvement of synovial structures are important to assess to determine what treatment is required. Simple wounds generally require only cleaning and bandaging to prevent infection, but deeper wounds may require suturing. Those potentially involving synovial structures should be assessed with distension of the joint or tendon sheath to determine whether communication occurs with the wound.
Diagnostics
Careful assessment of the wound, with cleaning to assess depth and any involvement of synovial structures. If significant blood loss is occurring, pressure bandaging is indicated to encourage clotting. If a synovial structure is potentially involved, the joint or tendon sheath should be sampled and synovial fluid collected for cytology, and culture and susceptibility testing. The synovial structure should then be distended with sterile fluid and communication with the wound assessed. If communication occurs, further flushing of the synovial structure is indicated. Suturing of the deeper areas of the wound may then be possible. Bandaging to keep the wound clean is also important.
Simple wounds do not require antimicrobial therapy, even if they are superficially contaminated. Topical wound care, including regular removal of biofilms, necrotic tissue and exudates, along with bandaging, is generally sufficient. Many topical wound therapies have been evaluated, but there is insufficient evidence to recommend one over another. Topical antimicrobials are not indicated. Wounds involving the distal limb can be slow to heal. Exercise restriction and bandaging can help to reduce the formation of excessive granulation tissue.
Deeper wounds that involve synovial structures should be flushed. Antimicrobial therapy is indicated, pending results of culture and susceptibility testing (see Synovial sepsis guideline).
Tetanus prophylaxis is critically important.
Good with appropriate therapy, unless infection of synovial structures occurs. Wounds on the distal limbs can be slow to heal and are prone to formation of exuberant granulation tissue. Wounds on the head and body tend to heal quickly and with fewer complications.
Hospitalised for 3 months.
Development of hypertrophic scars (common sequelae of deep 2nd-degree burns) on rump and hindlimbs.
Foaled a healthy filly foal 18 months after discharge from hospital.
Hoof abscesses occur more frequently following wet weather, when the sole of the hoof tends to be softer and more easily penetrated by foreign objects. Infection generally ascends from the solar corium (white line) and results in abscess formation. The accumulation of purulent exudate results in acute pain and non-weight bearing lameness in the affected leg. Mixed bacterial infection, including anaerobes, usually occurs due to inoculation of organisms from the environment into a relatively anaerobic area. Abscesses can drain through either the sole or coronary band.
Non-weight bearing lameness in one leg with an increased digital pulse. Pain is detected with hoof testers over the location of the abscess. Often there is a discoloured area of sole that can be pared with a hoof knife to allow drainage of the abscess.
If there are recurrent episodes of hoof abscessation in the same leg, radiographs are indicated to rule out infectious osteitis of the pedal bone (see chapter 2). Pars pituitary intermedius dysfunction (PPID) is another differential diagnosis in these cases and ACTH testing can assist in making a diagnosis, as long as seasonal and geographical reference ranges are used.
Drainage is key to resolution of the abscess. If the site to drain is not initially obvious, then bathing the hoof in hot water and poulticing it will aid in abscess localisation and establishing drainage.
Tetanus prophylaxis is required if the horse is not currently vaccinated for tetanus.
Excellent with rapid improvement following drainage of the abscess.
Septic pedal osteitis can be a sequela of penetrating wounds, subsolar abscesses and laminitis, where penetration of infection to the depth of the pedal bone can result in bone infection and formation of a sequestrum. Affected horses normally have a history of chronic lameness and drainage of purulent material from the hoof that does not resolve. Mixed bacterial infection, including anaerobes, is common due to inoculation from the environment into a relatively anaerobic area.
Detailed examination of the sole of the hoof for the site of penetration and purulent discharge is required. Radiographs of the hoof reveal decreased bone density, demineralisation and irregularity of bone margins at the level of the infected bone (1). Injection of contrast medium into the site of penetration may help to assess which structures are involved. It may take 7 days or longer for infection and sequestrum formation to result in radiographically detectable bone lysis. Examination of the hoof using computed tomography can be useful in difficult cases, to identify lytic areas of bone and small areas of sequestrum formation that are not evident on radiographs. Penetration of the navicular bursa and distal interphalangeal joint significantly worsens the prognosis.
Treatment requires a combination of surgical debridement of the infected bone and surrounding tissues, in addition to systemic and local antimicrobial therapy. Surgical debridement can be performed in the standing horse with appropriate sedation, regional anaesthesia, and the application of a tourniquet to control haemorrhage (2). The infected tissues are debrided, and the bone curetted and these samples should be submitted for culture and antimicrobial susceptibility testing. The defect is then lavaged and metronidazole is frequently used as a topical antimicrobial (1) before sterile bandaging. Systemic antimicrobials are continued until a healthy bed of granulation tissue has covered the pedal bone. Regional limb perfusions (see Section 12) are also frequently used. A treatment plate can be applied to protect the hoof and allow easy access for cleaning and flushing. Support for the opposite weight bearing foot by housing on sand, or use of soft-ride boots for frog support, is recommended to minimise the likelihood of support limb laminitis. Tetanus prophylaxis is required if the patient is not currently vaccinated for tetanus.
Septic pedal osteitis has a fair to good prognosis after surgical treatment, but there is a poorer prognosis without surgical debridement. The prognosis is guarded if the distal interphalangeal joint or navicular bursa are involved.
Street nail is a term describing a penetrating injury to the sole of the hoof. The site of penetration determines the severity of the injury, with an injury in the middle third of the frog most likely to result in penetration of the navicular bursa, which complicates treatment and significantly worsens the prognosis. Penetration to the depth of the pedal bone can also result in infectious osteitis and formation of a sequestrum. Horses quickly develop non-weight bearing lameness due to infection in the pedal bone and/or navicular bursa. Mixed bacterial infection, including anaerobes, is common due to inoculation from environment bacteria into a relatively anaerobic area. Historically, the procedure to establish drainage of the navicular bursa has been referred to as the ‘street nail procedure’ (3).
If the foreign penetrating body has been removed, detailed examination of the sole of the hoof should be performed to identify the site of penetration. Hoof testers are helpful to identify the site, as it will be painful on sole pressure. Radiographs are required to assess for pedal bone fracture. Injection of contrast medium into the site of penetration may help to assess which structures are involved. Infection and sequestrum formation can also be assessed with radiographs, but it may take 7 days or longer for bone lysis to occur and become detectable radiographically.
The area of the puncture should be opened and drained and the foot cleaned and poulticed. When penetration to the pedal bone is suspected, radiographs can be taken with contrast medium injected into the site of penetration.
If the penetrating object has penetrated the pedal bone or navicular bursa, surgery to curette the pedal bone and potentially flush the navicular bursa is required. A treatment plate can be applied to protect the hoof and allow easy access for cleaning and flushing.
Regional limb perfusion can also be used (see Section 12). Support for the opposite weight bearing foot by housing on sand, or the use of soft-ride boots for frog support, helps to minimise the likelihood of support-limb laminitis. Tetanus prophylaxis is required if the horse is not currently vaccinated for tetanus.
Guarded if the penetrating injury involves the navicular bursa. Infections of the pedal bone can also have a poor prognosis without surgical debridement.
When managing wounds, ensure horses are vaccinated for tetanus.
No antimicrobials therapy indicated, even if contamination of the wound is present.
Systemic antimicrobials only when:
Lavage is almost always required for a successful outcome. Systemic antimicrobials are always indicated. Therapy should be based on culture and susceptibility testing. Empirical therapy with penicillin and gentamicin should be initiated pending culture results.
Ensure horses are vaccinated for tetanus.
No antimicrobial therapy indicated.
Curette to establish drainage. If recurrent, consider the underlying disease. Radiographs should be taken to investigate for pedal osteitis, and ACTH measured to investigate for equine Cushing’s disease (PPID).
Systemic antimicrobials only when:
No obvious underlying cause. Often more severe than secondary cases.
An underlying cause can be identified (surgery, joint injection, wound, blunt trauma).
Fine-needle aspirate should be collected for culture and susceptibility testing. Care is needed for cellulitis occurring over synovial structures.
A document that outlines via a traffic light system, the different importance level of antimicrobials for use in horses.

The Australian Veterinary Prescribing Guidelines cattle and horse flipbook, detailing antimicrobials for use in cattle and horses.

The equine Australian Veterinary Prescribing Guidelines for antimicrobial use as a pocket guide booklet.

The equine Australian Veterinary Prescribing Guidelines poster. This document that outlines different antimicrobials for use in horses according to different diseases.
Funding for these guidelines was provided by the Australian Veterinary Association (AVA), Animal Medicines Australia (AMA) and AgriFutures Australia.
These guidelines would not have been possible without the considerable expertise and efforts of the Expert Panel: Associate Professor Laura Hardefeldt, Dr. Leanne Begg, Dr. Stephen Page, Professor Glenn Browning, and Professor Jacqueline Norris. We are also extremely grateful to the additional contributing authors.
The dedicated and skilled work of Project Manager Dr. Kellie Thomas is gratefully acknowledged, as are the contributions of the Project Steering Committee: Dr. Phillip McDonagh, Dr. John Messer, Professor James Gilkerson, and Dr. Melanie Latter. Open access publishing facilitated by The University of Melbourne, as part of the Wiley - The University of Melbourne agreement via the Council of Australian University Librarians.

![]()

Suggest a disease, syndrome or key evidence you think we should include.